 |
| I saw joggers outdoors through my window. I'll stay indoors, but I'll pedal... |
Saturday, January 4, 2014
Sunday, February 19, 2012
Weight loss – a new/old option
We all know the facts: Over two thirds of Americans are overweight. Half of them (one third of Americans) are medically obese, which places them at high risk for the development of premature heart attacks and a variety of other serious medical conditions.
The main cause of obesity is overeating, even more so than lack of physical activity.
The most effective way to lose weight is portion control, and with it comes the control of caloric intake.
But portion and calorie intake control is a tough job. It’s a “full time job,” and it takes willpower and discipline.
So what do you do when the brute force approach doesn’t work for you?
The New York Times Business section of February 16th had an interesting article on the possible approval by the FDA of a new appetite suppressant, Qnexa (U.S.
The use of appetite suppressants for the treatment of obesity has a long history. Medications like phentermine, Tenuate and Xenical have been used for years (we all remember the fen-phen period, of which phentermine emerged as the surviving drug…).
More recently, metformin (used in diabetes) has been used in some cases, and a combination of phentermine and certain antidepressants has been shown to be more effective than phentermine alone.
What’s new about Qnexa is not really new. The proposed drug is a combination of two well known medications now widely used: phentermine, the familiar appetite suppressant, and topiramate (Topamax) which is most commonly used for migraine prophylaxis.
Topamax, like most other drugs has a long list of side effects, one of which is weight loss. So physicians who treat obesity, have now begun using Topamax “off label” for it’s weight loss side effect, in combination with phentermine. The combination appears to be very effective.
The use of a medication for its side effects is not new. A good example is the wide use by hospitals of the Benadryl as a sleep medicine. In reality Benadryl (or its equivalents) is an antihistamine used for the treatment of allergies, and sleepiness as its most common side effect.
Whether Qnexa is actually approved by the FDA for weight loss or not, physicians are already using its components, the combination of phentermine and topiramate, to help patients lose weight when attempts at self control and lifestyle changes are not successful.
Wednesday, February 8, 2012
Want to lose weight? Choose a sign that fits your needs...

Found this picture in my travel album collection. Somewhere in Maine.
Sunday, November 27, 2011
Low Glycemic Index foods
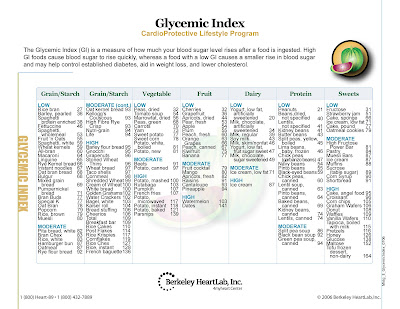
Low Glycemic Index (GI) may help you control your appetite. The table below, published by Bekeley Heart Lab, Inc., shows the GI of some common foods. Look at it carefully, and I'm sure you'll find some unexpected results. Always try to choose the foods with the lowest GI. For example, when looking for a fruit snack, choose cherries or grapefruit over watermelon or dates.
As a reference, the GI of table sugar (and corn syrup) is approximately 90.
Berkeley Heart Lab is known for its in-depth analysis of blood cholesterol profile and the resulting cardiac implications. We use their services when appropriate.
To enlarge the GI chart, just click on the image. You can also click and drag it to your desk top.
As a reference, the GI of table sugar (and corn syrup) is approximately 90.
Berkeley Heart Lab is known for its in-depth analysis of blood cholesterol profile and the resulting cardiac implications. We use their services when appropriate.
To enlarge the GI chart, just click on the image. You can also click and drag it to your desk top.

Tuesday, October 25, 2011
Eat low Glycemic Index foods
The Glycemic Index (GI) of a food is a measure of how much blood sugar level rises after eating a given amount of that food. The lower the GI of a given food, the lower will be the rise in your blood sugar. Your pancreas will not be called upon to release insulin as fast, and several benefits accrue: better control of blood sugar levels, a decrease in appetite, better weight control, and a lower risk of developing full fledged diabetes.
As a reference point, the Glycemic Index of table sugar is 64 (not very good), and for some foods it can exceed a real-bad 130 (dates, French baguette and, yes, non-dairy tofu frozen desert).
Here are some examples of the good, the mediocre, and the bad (note: this is only a guideline; for the actual values of many foods, click here):
Low Glycemic Index foods, 55 or less, good: Milk (skim or fat), plain yogurt, legumes (lentils, kidney beans, chick peas), soy beverages, certain fruits (apples, plums, grapefruit, oranges, berries), oat bran bread, pumpernickel bread, slow cooked oats (oatmeal), whole grain pasta (al dente is better, believe it or not…).
Medium Glycemic index foods, 55-69, mediocre: Banana, pineapple, raisins, new potatoes, split pea or green pea soup, brown rice, All-Bran™, shredded wheat cereal, whole wheat bread, rye bread.
High Glycemic index foods, 70 or more, not so good): White bread or bagel, white potatoes, parsnips, rutabaga, instant rice, certain cereals (Cheerios™, Corn Flakes™, Rice Krispies), french fries, ice cream, table sugar, jelly beans, watermelon, naturally sweetened sodas.
Need more information and/or support? Give us a call.
Monday, October 24, 2011
Lose weight with an HMR shake for breakfast
When we need to lose a few pounds, Sandy and I find it helpful to control our breakfast calorie intake by using HMR shakes. We prefer the HMR 70 vanilla mix. This is how we use it:
1 packet of HMR 70 vanilla mix
1 glass filled ½ with crushed ice & ½ with water
1 tsp Hershey’s powdered cocoa (sugar-free)
Place HMR packet in bottom of blender.
Add ice, water and cocoa, and blend.
Optional additions:
½ banana or,
½ cup berries
flavor extracts (calorie free)
Add to partially-blended shake and blend again for an additional minute. Enjoy!
Calories:
HMR 70, 110 calories
Banana/berries, 50 calories (approx)
Hersheys cocoa, 5 calories
Total 165 calories (approx)
You may use 1 ½ to 2 packets of HMR, but remember to count your calories. You may experiment with other fruits and extracts to create the shake you like best.
HMR shakes and other weight loss foods are available at our office. They are an integral part of our medically supervised weight loss program.
Sunday, July 31, 2011
Weight and antidepressants - what's the connection?
Does the use of antidepressants affect your weight?
For many, this is a valid health question. For others, especially women (but not limited to women), it's also a social issue, a body-image issue, and many times a reason for refusing to use medically-necessary antidepressant medication.
Many patients on antidepressants gain weight. Is it a direct effect of the antidepressant, or is it that some patients begin to enjoy life more, and "celebrate" it with more eating?
Others lose weight. Is this a direct effect of the medication, or is it that these patients can now better deal with the realities of life and better control their eating habits and exercise?
While the jury is still out on this question, some answers begin to emerge. A meta-analysis (a statistical analysis of related research) that appeared in October of last year in the respected Journal of Clinical Psychiatry indicates that the antidepressants Amitriptyline (Elavil) and Mirtazapine (Remeron) and Paroxetine (Paxil) are associated with weight gain, while the antidepressants Ffluoxetine (Prozac) and Buproprion (Wellbutrin) are probably associated with weight loss.
The pressure to treat overweight in both depressed and non-depressed patients has become so urgent that some antidepressants are now used "off label" for weight loss, either alone or in combination with prescription appetite suppressants.
So, if you're taking or contemplating the use of an antidepressant, and weight loss or weight gain is an issue for you, don't forget to discuss the specific pros and cons related to your situation, with your doctor.
In our office, we have the ability to make a very reliable estimate of your daily caloric requirements (we do this by measuring your actual oxygen consumption while at rest), and use that as a guide in treatment when a combination of depression and obesity exists.
Subscribe to:
Posts (Atom)